
Our Favorite Subject: Fat(ty Acids)s
PODCAST TRANSCRIPT OF "OUR FAVORITE SUBJECT: FAT(TY ACIDS)S": {Listen now}. Click on the pictures to enlarge them.
Hello and thanks for joining me. My name is Ayn Devera, I’m a Human Nutritionist, and the director and owner of Inner Soulstice Wellness Movement and Health Studio, located in beautiful Ventura, California.
Welcome to my first podcast demystifying the macronutrient, fat. I’ll be primarily discussing the essential fatty acids (EFAs), Omega 6 and Omega 3. Some of it will be very science-oriented, but here’s the thing, I think it’s really important to empower you with the why because it becomes more valuable to you as a tool for your health. To make this information more digestible, I’ve included the transcript below with pictures to help you visualize what I’m talking about.
I’m going to review how the structure and function of cells are affected by the ratio of foods you eat that are higher in Omega 6 than Omega 3. First, I want to clear the misinformation about fats. Fats are not all functionally the same, and really should be viewed as neither bad nor good, but rather by how they operate in our bodies to induce health over detriment.
So let’s get to it!
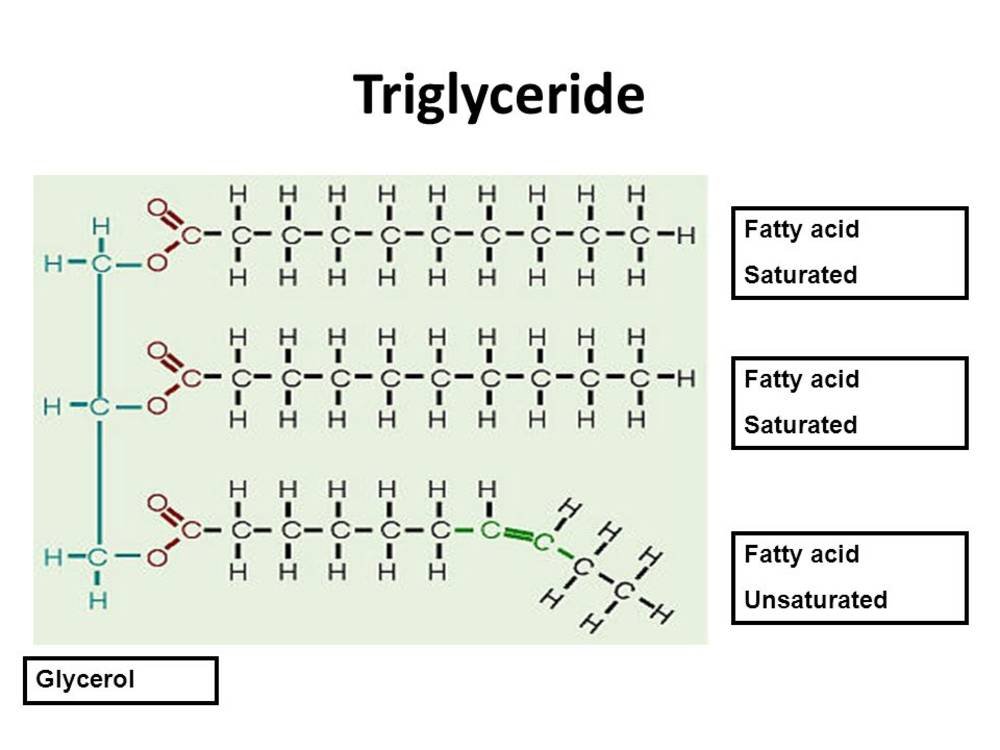
The actual shape of a fatty acid, such as saturated fats and polyunsaturated fats, contributes to a cell’s structure and function. The bends and kinks created by double bonds within a carbon chain (polyunsaturated fats or PUFAs for short) make the fatty acid flexible, whereas no kinks (saturated fats), create rigidity. In my transcript, you’ll see a picture of a triglyceride composed of a glycerol backbone, two saturated fats capped by a hydrogen, and a polyunsaturated fat with a double carbon bond where the kink occurs. Both types are needed in the phospholipid bilayer of our cell membranes for structure and fluidity of the cells, and appropriate membrane functions such as permeability, receptor function, and intracellular signaling. Let me break it down further.

We need both types, saturated and unsaturated fatty acids, to create flexible, yet sturdy cell membranes. A key thing to remember, is everything in our body is made up of cells and the structure of the cell membrane determines how it’s going to function. Flexible fatty acids promote flexible tendons, muscles, and other tissues. If the phospholipid bilayer of the cell membranes had more saturated carbon chains on the other hand, then the cell membrane would be harder, less permeable, with reduced receptor function, and intracellular signaling. Think of atherosclerosis, the hardening of arteries. We still need saturated fats, however, because they’re dense and provide structure. The bottom line is a balance and an understanding of how our bodies metabolize Omega 6 and Omega 3 is needed.



So, we’ve covered a little bit about how structure determines function, and why both saturated fats and polyunsaturated fats are integral to the composition of the cell membrane. The second topic regarding the appropriate Omega 6 to Omega 3 ratio I’ll be talking about is how they affect all local inflammatory responses in the body 20-carbon essential fatty acids. These are Di-Homo-Gamma Linolenic Acid (DGLA) an Omega 6, Arachidonic Acid (AA) also an Omega 6, and Eicosapentaenoic Acid (EPA) an Omega 3, and depending on their ratios, they can give rise to either anti-inflammatory eicosanoids known as Series 1 & 3 prostaglandins and thromboxanes, or inflammatory Series 2 & 4 eicosanoids. Eicosanoids are local hormones that either bring on or reduce inflammation. They also regulate smooth muscle contraction and relaxation- such as in the blood vessels, bronchioles, and GI tract. In short, more inflammatory eicosanoids give rise to inflammatory diseases such as cardiovascular, autoimmune diseases, and symptoms such as headaches and allergies.
Foods in the Omega 6 family such as vegetable oils, grains, animal products, and shellfish are consumed on a larger scale than foods in the Omega 3 family, such as coldwater fish, flaxseed oil and walnuts. In fact, the Standard American Diet involves a ratio of Omega 6 food to Omega 3 food consumption of approximately 25:1. In other parts of the world this ratio is about 4:1. A higher Omega 6 intake promotes the pro-inflammatory cascade of eicosanoids. This can explain the high rates of cardiovascular disease, cancer, and autoimmunity in the U.S.
So, the question still remains how? Well, in our bodies, Omega 6 and Omega 3 share the same pool of enzymes that metabolize short chain fatty acids to their end products, either inflammatory Arachadonic Acid, or anti-inflammatory Eicosapentaenoic Acid, EPA for short, and Docosahexaenoic Acid, also referred to as DHA.
Arachidonic Acid is a long chain carbon fatty acid that is derived from the short chain fatty acid, Linoleic Acid. Both are Omega 6 fats. The Omega designation of 3 or 6 is for another lecture, but basically has to do with how many and where the double carbon bonds land in the carbon chain. When we consume more Linoelic Acid (canola, corn, soybean, safflower, sunflower oils) than Alpha Linolenic Acid (flaxseed, hemp, walnut oils), the Delta 6 Desaturase enzyme converts it to Gamma Linolenic Acid, which uses the Elongase enzyme to convert it to Di Homo Gamma Linolenic Acid, which then uses the Delta 5 Desaturase enzyme to form Arachidonic Acid.

When we consume more Alpha linolenic acid, then the Delta 6 and Delta 5 Desaturases and Elongase enzymes will be pulled toward creating more anti-inflammatory products such as EPA and DHA.

Now, Di Homo Gamma Linolenic Acid can go in two different pathways. Derived from Linoleic acid via Delta 6 Desaturase and Elongase, it can go all the way to Arachidonic Acid. Or we can stop it in its tracks, and push it toward EPA and DHA production by supplementing our diet with flax. I’ve included a great illustration of this inflammatory cascade showing how DGLA can be diverted from becoming Arachidonic Acid. Remember, Arachidonic Acid with give rise to inflammatory products.

It’s so important to promote EPA and DHA in our diet. This duo has been shown to have cardio protective benefits, reducing coronary plaque and inhibit the progression of atherosclerosis. Omega 3 fatty acids have been shown to prevent sudden cardiac death by blocking fatal heart rhythms, and DHA which is predominantly found in the eyes and brain, has been associated with a reduced risk of developing all-cause dementia. DHA can also slow down the progression of macular degeneration.
We can also consume EPA and DHA in our diet in the form of fish oil. Part of the reason we supplement with Omega 3 is because it can have higher purity and safety than fish. One serving, according to the EWG, of farmed salmon can have 40 times more PCBs (polychlorinated biphenyls, highly toxic industrial compounds) that can cause serious neurological health risks to fetuses. One can of tuna contains 530 mg of EPA/DHA, but due to mercury levels, one can per week is recommended, which requires the need for other foods sources for EPA/DHA.

A deficiency of Omega 6 in the diet can lead to dermatitis, scaly skin, eczema, bumpy skin (chicken skin texture on the back of arms), and acne. An Omega 3 deficiency can lead to eye diseases, trouble concentrating, and heart disease. A lot can be managed with appropriate essential fatty acids in the diet and some telltale signs of balance found in the skin and brain function. Abnormal metabolism of essential fatty acids can occur in Cystic Fibrosis, Crohn’s Disease, cirrhosis, alcoholism, and Reye’s syndrome.

Resource:
Lindner, S. (2013). Lecture 3: Fats [PowerPoint slides]. Retrieved from University of Bridgeport, Vitamins and Minerals
Nutritional Support for Delta 6 Desaturase
Nutritional Support for Delta 5 Desaturase
Learn more